This informal CPD article ‘The Hyoid Bone: Biomechanical Analysis of a Mechanical Convergence Point - Force Redistribution in the Cranio-Cervical District’, was provided by Dr. Mauro Lastrico, Physiotherapist at AIFiMM Formazione, an organisation recognised by the Italian Ministry of Health as an authorised CME provider. They offer organised training courses in the Mézières Method, a rehabilitative and postural approach.
This article is part of a series dedicated to applying the principles of physics to the musculoskeletal system. The article Clinical Assessment of Muscle Shortening [1] introduced the physical model of muscle shortening as viscoelastic deformation of connective components, distinguishing the mechanical behaviour of the contractile component from that of the connective component.
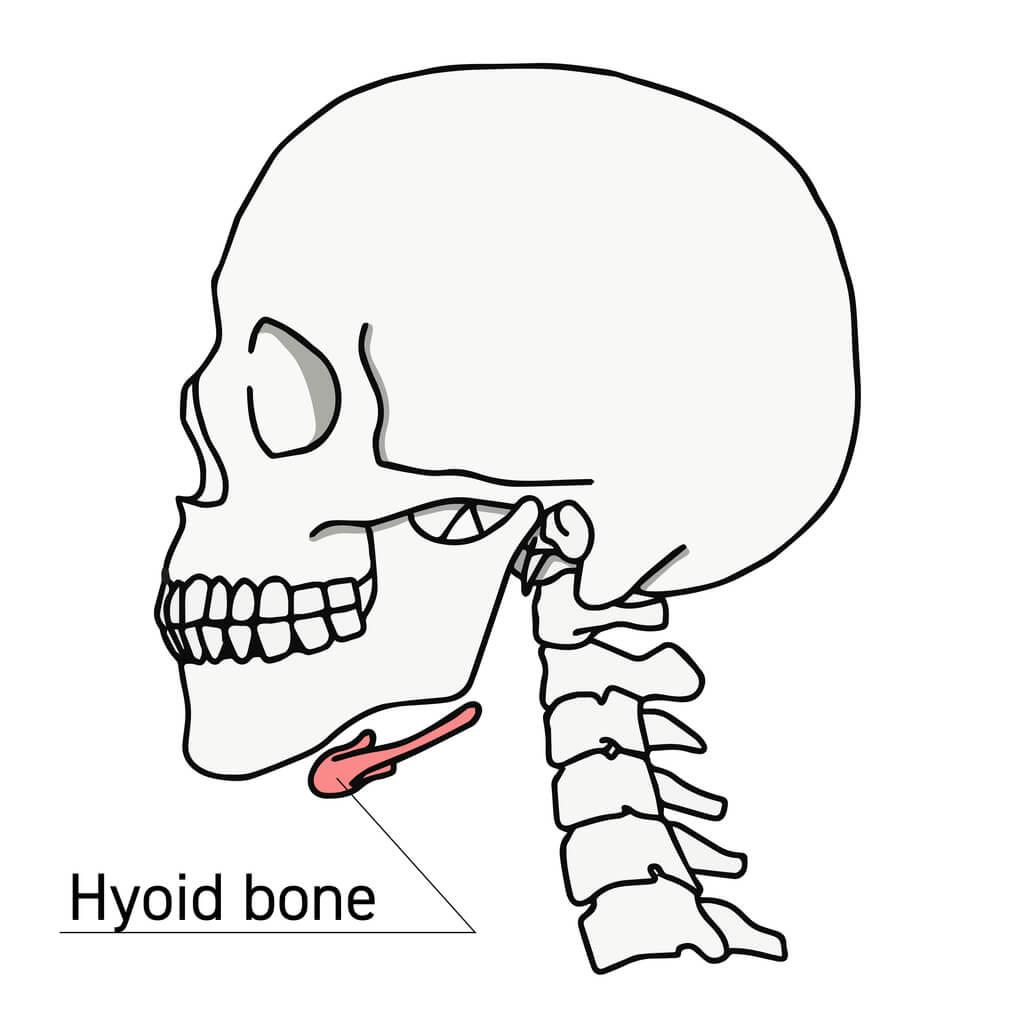
The present work applies these principles to the analysis of the hyoid bone, a peculiar anatomical structure that, lacking articulations with other skeletal segments, represents a mechanical convergence point of muscular forces. Understanding its biomechanical behaviour enables interpretation of symptomatologies in the cranio-cervical district that may derive from distant muscular tensions, propagated through the anatomical connections converging on this element [1,2].
1. Anatomy and Biomechanical Characteristics
In the analysis of the musculoskeletal system, muscular forces determine the positioning of skeletal segments through their osseous insertions [2,3]. The hyoid bone represents a particular case in this biomechanical analysis: it is completely suspended in the anterior region of the neck, maintained in position exclusively through a complex system of muscular and fascial connections [4,5].
This condition of total suspension renders the hyoid bone a peculiar anatomical element. Unlike skeletal structures for which articulations provide precise mechanical constraints, the position of the hyoid bone in space is determined uniquely by the equilibrium of muscular forces converging upon it [5,6].
This anatomical characteristic produces several biomechanical consequences: the hyoid bone becomes the point of mechanical convergence of six muscular systems originating from the cranium, mandible, sternum, scapula, larynx and pharynx [4,7]. Through these connections the hyoid bone participates as a passive element in complex functions: it is mobilised during movements of mandibular opening, during swallowing and phonation, follows respiratory movements and adapts to variations in cranio-cervical axes and scapular position [7,8].
2. The Hyoid Bone as a Point of Force Convergence
The hyoid bone is situated at the centre of a system of muscular forces originating from the cranium, mandible, sternum and scapula, and its position in space is determined by the vectorial equilibrium of all these converging forces [2,5]. When tension varies in any of the inserted muscles - through shortening of connective components according to the mechanisms previously analysed [1] - the equilibrium of forces is altered and the bone is passively displaced to a new position.
This displacement induces the other muscles of the system to increase their tone to adapt to the new geometry and, being connected to other skeletal districts, the tensional alterations propagate to the cranium, mandible, cervical vertebrae and scapula [9,10]. This is not an active transmission: the hyoid bone passively undergoes the action of applied forces and its new position determines the mechanical conditions for the redistribution of tensions throughout the entire district.
Due to this mechanical characteristic it can be considered a nodal point of the cranio-cervico-scapular system [10,11]. It is important to emphasise that the hyoid bone exerts no regulatory nor autonomous functional action: every positional variation represents the passive resultant of the equilibrium of muscular forces converging upon it [2,5].
2.1 Systemic Integration
The muscles inserting on the hyoid bone form part of the muscular system that functionally connects the cranium, cervical column, thorax and pelvis [12]. When tension varies in one district, this propagates mechanically through anatomical connections. The hyoid bone functions as a mechanical relay: it neither generates nor amplifies signals, but represents the point through which tensional variations are redistributed.
As in an electrical relay where variation in one circuit influences connected circuits, so the tensional modifications reaching the hyoid bone through one muscle group determine mechanical variations in all other inserted muscles [2,11]. From the scapula and sternum depart muscles directed cranially towards the cervical vertebrae and cranium, and caudally towards the thoraco-lumbar vertebrae and pelvis. The hyoid bone, through its direct and indirect connections, participates in this force distribution network [12,13].
A tension originating from the scapular region can thus mechanically influence the mandibular district, and vice versa [10,13]. This mechanism of tension propagation explains why apparently local symptomatologies may derive from distant biomechanical causes [14].
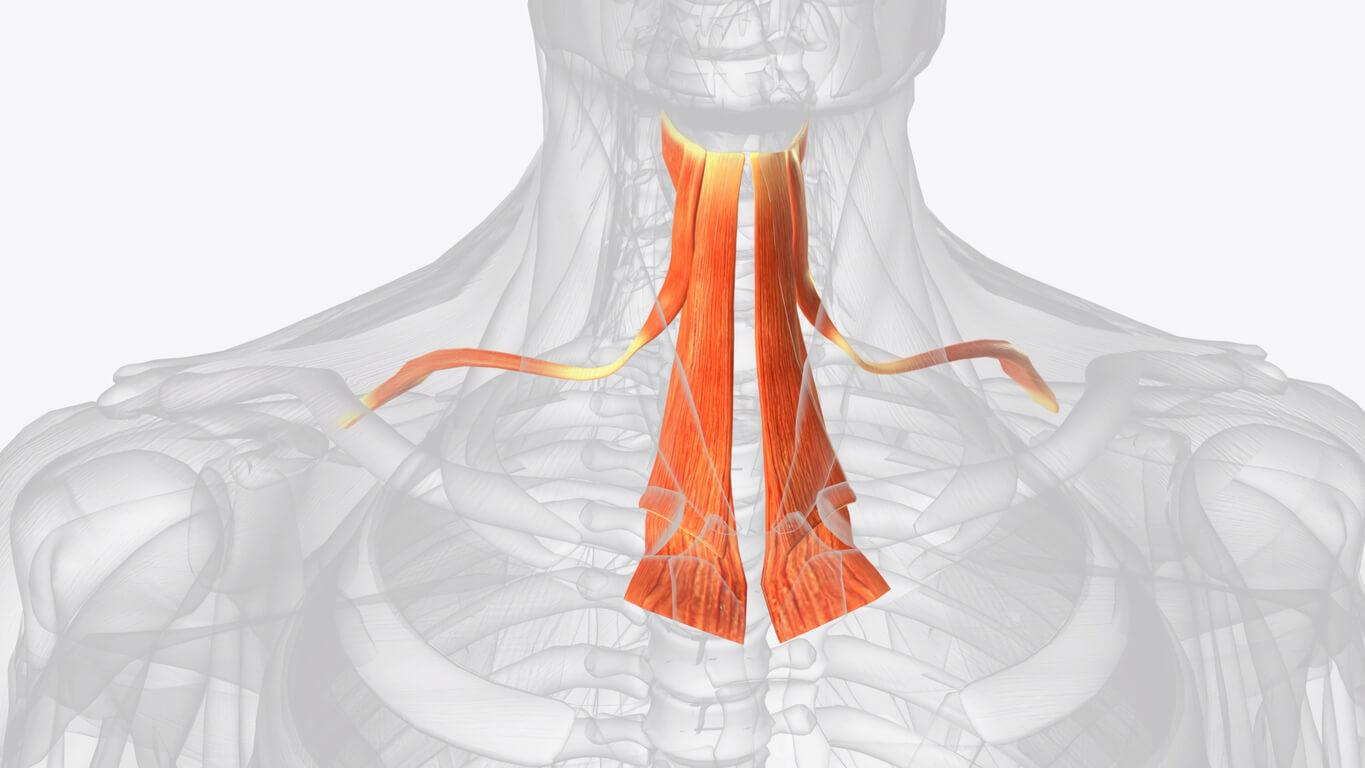
Infrahyoid muscles
3. Force Analysis: Dominance of Suprahyoid Muscles
Vector analysis of the hyoid system shows a clear dominance of suprahyoid muscles over infrahyoid muscles: the digastric, stylohyoid, geniohyoid and mylohyoid muscles are indeed more numerous and present superior force vectors [5,15]. Their lines of force, moreover, have more favourable angulations for traction in cranial and anterior directions [15].
The infrahyoid muscles - sternohyoid, omohyoid, thyrohyoid - result subdominant. Their capacity to counter superior traction is limited both by reduced number and by less favourable vectorial disposition [5,15]. When excessive tensions develop in any district connected to the hyoid bone, the dominance of the suprahyoid muscles determines its elevation and anteriorisation through the prevalent action of the anterior digastric [16].
If omohyoid tension is asymmetric, lateral deviation may also be added and all muscles inserted on the hyoid mechanically modify their tensional state [17]. In cascade the infrahyoid muscles react by increasing their tension in an attempt to counter the elevation but, being subdominant, they cannot restore the bone to neutral position [2,15].
Compensations are thus created that propagate to connected districts through common muscular insertions [10,14]. This compensation pattern explains why a true lowering of the hyoid bone is rarely observed in clinical practice, given the vectorial dominance of the suprahyoid muscles [15,18].
4. Functional Consequences of Suprahyoid Dominance
When hyoid muscles enter excessive tension and subsequent shortening [1], the altered position of the hyoid bone determines functional modifications in the processes of swallowing, phonation and respiration [7,8,19].
4.1 Alterations of Swallowing
In physiological swallowing the hyoid muscles work in synergism with the mandibular closing muscles [20]. Occlusal problems or cranio-cervical musculoskeletal imbalances can interfere with correct balancing between the two muscle groups, determining phenomena of atypical swallowing [20,21]. The stable elevation of the hyoid bone alters the geometry of the mandible-hyoid-larynx complex, modifying muscle activation patterns during swallowing [21].
4.2 Alterations of Phonation
Variations in vocal frequency depend on laryngeal position: for emission of high-pitched sounds the larynx rises through action of the suprahyoid muscles, for low-pitched sounds it descends through action of the infrahyoid muscles [22]. The hyoid bone, connected to the larynx through the thyrohyoid membrane and thyrohyoid muscle, participates passively in these movements [7,22].
With the hyoid bone stably elevated due to suprahyoid dominance, caudal excursion of the larynx is therefore limited [22,23]. The voice tends towards high frequencies - not in volume but in timbre - with reduced capacity for modulation and the constant excess of muscular tension can determine vocal fatigue [23,24].
4.3 Alterations of Respiratory Mechanics
During physiological inspiration, the hyoid bone should accompany the descent of the diaphragm through the action of infrahyoid muscles, then return to neutral position during expiration [25]. With the hyoid bone stably elevated due to suprahyoid dominance, the caudal inspiratory movement may be limited or absent [25,26].
The infrahyoid muscles, already in tension attempting to counter the elevation, cannot effectively mobilise the bone downwards. The bone remains fixed in elevated position instead of following the respiratory rhythm, interfering with physiological respiratory mechanics [26,27].
4.4 Alterations of Cranio-Cervical Axes
The tensions of muscles connecting the hyoid bone to cranium and scapula participate in maintaining cranio-cervical axes [9,28]. The altered position of the bone mechanically modifies the tensions of all muscles in the district, contributing to modifications of cranial position, alterations of cervical curves and cranio-cervical tensional asymmetries [28,29]. The anteriorisation of the hyoid bone determines anterior traction on the middle cervical vertebrae, particularly C3-C4, modifying physiological cervical lordosis [29].
Assessment of the hyoid bone
5. Clinical Assessment
Assessment of the hyoid bone provides information on the tensional state of the system [18,30]. On direct palpation the hyoid bone should theoretically be located midway between the inferior mandibular margin and the thyroid prominence. In clinical practice it is often found elevated, due to suprahyoid dominance: therefore its distance from the inferior mandibular margin is assessed as well as symmetry relative to the midline [18,30].
During swallowing its vertical and anterior excursion is observed and during phonation the positional variations with changes in vocal frequency [20,22]. The elevated and anteriorised position of the hyoid represents the most frequent picture and indicates excess tension of the suprahyoid muscles [18,30].
This alteration of the cervical axis is associated with tensions in the mandibular district and cranial base, limitation of caudal excursion of the bone, tendentially high-pitched vocal frequency and possible atypical swallowing [21,23,29]. Lateral deviation signals asymmetry of tensions on the two sides, generally due to unilateral traction of the omohyoid consequent to scapular region imbalances [17].
A true lowering of the hyoid bone is rarely observed, given the vectorial dominance of the suprahyoid muscles [15,18]. Palpatory assessment should be integrated with functional observation during swallowing, phonation and respiration to understand the overall biomechanical picture [30].
Conclusions
The hyoid bone, lacking articulations with other skeletal segments, represents a mechanical convergence point of muscular forces originating from the cranium, mandible, sternum and scapula. Its position in space reflects the equilibrium of these forces [2,5].
Vector analysis shows a dominance of suprahyoid muscles which determines, in cases of tensional alterations, a characteristic pattern: elevation and anteriorisation of the bone, with possible lateral deviations but not true lowerings [15,18]. The alteration of hyoid bone position produces direct mechanical consequences: modification of cervical lordosis through anterior traction on middle vertebrae, alterations of swallowing and phonation, interferences with respiratory mechanics [7,19,29].
Understanding the role of the hyoid bone as a point of mechanical redistribution of tensions enables interpretation of symptomatologies in the cranio-cervical district that may derive from distant muscular tensions, propagated precisely through the anatomical connections converging on the bone [10,14]. This biomechanical approach provides an interpretive tool for clinical assessment, enabling identification of primary causes of functional alterations rather than limiting treatment to local symptoms [1,2,30].
We hope this article was helpful. For more information from AIFiMM Formazione, please visit their CPD Member Directory page. Alternatively, you can go to the CPD Industry Hubs for more articles, courses and events relevant to your Continuing Professional Development requirements.
References
1. Lastrico M. Clinical Assessment of Muscle Shortening. The CPD Certification Service; 2025.
2. Winter DA. Biomechanics and Motor Control of Human Movement. 4th ed. Hoboken: Wiley; 2009.
3. Lieber RL, Fridén J. Functional and clinical significance of skeletal muscle architecture. Muscle Nerve. 2000;23(11):1647-1666.
4. Pearson WG Jr, Langmore SE, Zumwalt AC. Evaluating the structural properties of suprahyoid muscles and their potential for moving the hyoid. Dysphagia. 2011;26(4):345-351.
5. Van Eijden TM, Korfage JA, Brugman P. Architecture of the human jaw-closing and jaw-opening muscles. Anat Rec. 1997;248(3):464-474.
6. Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383-389.
7. Moon JB, Canady JW. Effects of gravity on velopharyngeal muscle activity during speech. Cleft Palate Craniofac J. 1995;32(5):371-375.
8. Dodds WJ, Stewart ET, Logemann JA. Physiology and radiology of the normal oral and pharyngeal phases of swallowing. AJR Am J Roentgenol. 1990;154(5):953-963.
9. Rocabado M. Biomechanical relationship of the cranial, cervical, and hyoid regions. J Craniomandibular Pract. 1983;1(3):61-66.
10. Page P, Frank CC, Lardner R. Assessment and Treatment of Muscle Imbalance: The Janda Approach. Champaign: Human Kinetics; 2010.
11. Myers TW. Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists. 3rd ed. Edinburgh: Churchill Livingstone; 2014.
12. Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndromes. St. Louis: Mosby; 2002.
13. Hackney ME, Moffat M. Muscle imbalance in the cervical spine: a review of anatomy, kinesiology, and therapy. J Dance Med Sci. 2007;11(1):20-27.
14. Lewit K. Manipulative Therapy in Rehabilitation of the Locomotor System. 3rd ed. Oxford: Butterworth-Heinemann; 1999.
15. Perlman AL, Palmer PM, McCulloch TM, Vandaele DJ. Electromyographic activity from human laryngeal, pharyngeal, and submental muscles during swallowing. J Appl Physiol. 1999;86(5):1663-1669.
16. Cook IJ, Dodds WJ, Dantas RO, Kern MK, Massey BT, Shaker R, Hogan WJ. Timing of videofluoroscopic, manometric events, and bolus transit during the oral and pharyngeal phases of swallowing. Dysphagia. 1989;4(1):8-15.
17. Ackland DC, Pak P, Richardson M, Pandy MG. Moment arms of the muscles crossing the anatomical shoulder. J Anat. 2008;213(4):383-390.
18. Matsubara K, Kuang-Hsien H, Nozaki S, Omori K. A computed tomographic study of the hyoid bone and its correlation with facial morphology. J Oral Rehabil. 2007;34(8):594-598.
19. Palmer JB, Rudin NJ, Lara G, Crompton AW. Coordination of mastication and swallowing. Dysphagia. 1992;7(4):187-200.
20. Logemann JA. Evaluation and Treatment of Swallowing Disorders. 2nd ed. Austin: Pro-Ed; 1998.
21. Fujiki RB, Thibeault S, Todey E. Physiological characteristics and perceptual outcomes of atypical swallowing. J Speech Lang Hear Res. 2017;60(11):3227-3239.
22. Honda K, Hirai H, Masaki S, Shimada Y. Role of vertical larynx movement and cervical lordosis in F0 control. Lang Speech. 1999;42(4):401-411.
23. Titze IR. Principles of Voice Production. 2nd ed. Iowa City: National Center for Voice and Speech; 2000.
24. Roy N, Merrill RM, Gray SD, Smith EM. Voice disorders in the general population: prevalence, risk factors, and occupational impact. Laryngoscope. 2005;115(11):1988-1995.
25. Ayoub MR, Spengler DM, Martin JW. The external oblique muscle electromyographic analysis in loading and unloading of the trunk. Ergonomics. 1975;18(5):545-552.
26. Mead J, Agostoni E. Dynamics of breathing. In: Fenn WO, Rahn H, editors. Handbook of Physiology: Respiration. Washington: American Physiological Society; 1964. p. 411-427.
27. De Troyer A, Estenne M. Coordination between rib cage muscles and diaphragm during quiet breathing in humans. J Appl Physiol. 1984;57(3):899-906.
28. Vasavada AN, Li S, Delp SL. Influence of muscle morphometry and moment arms on the moment-generating capacity of human neck muscles. Spine. 1998;23(4):412-422.
29. Harrison DD, Janik TJ, Troyanovich SJ, Harrison DE, Colloca CJ. Evaluation of the assumptions used to derive an ideal normal cervical spine model. J Manipulative Physiol Ther. 1997;20(4):246-256.
30. Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and Function with Posture and Pain. 5th ed. Baltimore: Lippincott Williams & Wilkins; 2005.