This informal CPD article ‘Vector Analysis in Musculoskeletal Biomechanics - Part 1: Foundations and Clinical Principles’, was provided by Dr. Mauro Lastrico, Physiotherapist at AIFiMM Formazione, an organisation recognised by the Italian Ministry of Health as an authorised CME provider. They offer organised training courses in the Mézières Method, a rehabilitative and postural approach.
Introductory Note
This article represents the third contribution in a series dedicated to applying the principles of physics to the musculoskeletal system. The first article, Clinical Assessment of Muscle Shortening [1], introduced the physical model of muscle shortening as viscoelastic deformation of the connective components, distinguishing the mechanical behaviour of the contractile component from that of the connective component. The second article, Body Equilibrium – A Physical-Clinical Interpretation of Human Upright Stability [2], presented the interpretation of human equilibrium as alignment between the weight force (G) and the ground reaction force (R), refuting the concept of "antigravity muscles".
The present article completes the theoretical framework by introducing vector analysis as a tool for identifying the muscular causes of alterations in physiological joint sequence. This is part one of a two-part article with the second part addressing Clinical Applications and Case Interpretation. Through this approach, it is possible to translate anatomical complexity into interpretable and clinically applicable mathematical models [3,4].
The objective is not to propose an alternative paradigm to evidence-based physiotherapy, but to provide an interpretive tool that allows us to understand why certain joint alterations manifest with predictable patterns, and how to direct therapeutic intervention towards primary causes rather than secondary manifestations [4,5].
1. Muscles as Traction Forces
The biomechanical analysis proposed here involves transforming muscle fascicles into lines of traction force, to which their respective vectorial actions on skeletal components are applied [3,5].
Muscles work exclusively through traction forces, bringing insertions closer together during contraction [6,7]. This statement, apparently obvious, has profound implications for clinical assessment: it means that every muscle, regardless of its traditionally attributed function, exerts a force that pulls its insertions towards each other [6].
The direction of this traction is not arbitrary: it is determined by the anatomical arrangement of muscle fibres and can be represented as a vector [7,8]. When a muscle contracts or when its connective components are shortened, this traction force manifests constantly, modifying the geometric relationships between skeletal segments [1,6].
Anatomical structures such as the patella or malleoli do not contradict this principle: they function as pulleys that redirect the direction of traction, not as points of application of different forces [6,9]. The patella, for example, modifies the angle of quadriceps traction on the tibia, but the nature of the force remains a traction exerted by the muscle on its insertions [9].
2. The Vector: Definition and Characteristics
In physics, a vector is a geometric element characterised by three fundamental properties [10,11]. Understanding these properties is essential for applying vector analysis to musculoskeletal assessment.
Magnitude: represents the intensity of the force, graphically expressed by the length of the vector segment. Clinically, it corresponds to the extent of muscular force, which depends both on the contractile capacity of the muscle and on the passive tension of its connective components [1,3,10]. A muscle with shortened connective components exerts a traction force even in the absence of active contraction [1,8].
Direction: the line on which the vector lies. Anatomically, it corresponds to the line of force of the muscle, determined by the arrangement of its fibres [7,12]. A muscle with parallel fibres, such as the sartorius, has a well-defined vectorial direction; a pennate muscle, such as the deltoid, has a resultant direction from the sum of the vectors of individual components [7,12].
Sense: the orientation along the line, graphically expressed with an arrow. It indicates the direction of muscular action, from origin towards insertion during contraction [6,7]. Since muscles can pull both insertions (unless one is fixed by other muscles or by the skeleton), the sense can be bidirectional [6].
A vector is indicated by an oriented segment from point A to point B. Two vectors can have the same direction but different magnitudes (same line of force, different intensities), or the same direction and magnitude but opposite sense (equal and opposite forces) [10,11].
3. The Parallelogram Rule and Vector Addition
Through the parallelogram rule, it is possible to calculate the resultant of two or more vectors [10,11]. This mathematical principle, fundamental in physics, finds direct application in musculoskeletal biomechanics.
From a clinical perspective, the parallelogram rule allows us to: predict the resultant movement from the combined action of multiple muscles; identify which muscles are responsible for an observed dysmorphism; understand the compensatory mechanisms that the neuromuscular system implements to maintain equilibrium [3,4,10].
In systems with many acting forces, to arrive at the overall resultant, forces are added two by two, always applying the parallelogram rule [10]. This methodical approach guarantees the reproducibility and objectivity of clinical assessment [4,13].
The parallelogram rule is also used for the inverse process: calculating the intensity that one or more vectors must express to balance another based on their spatial arrangements [10,11]. A vector can be balanced by a vector having the same magnitude but opposite direction, or by two or more oblique vectors whose modular sum equals that of the vector to be balanced [2,10].
This application is clinically crucial: when a muscular force increases (through active contraction or through shortening of connective components), other forces must necessarily activate to maintain joint equilibrium [2,14]. If this balancing does not occur, the skeletal segment moves in the direction of the dominant force [2,4].

Muscular force increases
4. Force Couples and Resulting Moments
Vector addition does not always produce a single resultant, especially when considering the three-dimensional plane. When at least two non-aligned resultants are present, we speak of a "force couple" [10,11].
Force couples generate resulting "moments" [3,10]. The total moment of force is given by the sum of the product between the magnitudes of the forces and their half-distance. Moments determine joint rotations and load concentrations that can generate localised overloads [3,15].
A clinical example is represented by the force couple exerted on the scapula by the lower fibres of the trapezius and the teres major: these two forces, distant from each other and with non-parallel directions, create a rotational moment on the scapula that determines its combined movement of rotation and tilting [12,16]. Understanding these moments is essential for interpreting the alterations in scapular kinematics observed in impingement syndromes [16,20].
5. The Importance of Vector Obliquity
A parameter of vector analysis, often underestimated in traditional clinical assessment, is the obliquity with which force acts relative to the skeletal segment [7,12].
When two diagonal forces maintain a skeletal segment vertical, if they have different angulation relative to the segment, they must use asymmetric intensities to achieve balance [3,10]. The force with greater angulation (more oblique) is mechanically "advantaged": at equal intensity, it produces greater displacement of the segment [3,5].
The segment bends in the direction of the more oblique force when the vectorial balancing capacity of the force with lesser angulation is exceeded [3,5]. This principle explains why apparently "weaker" muscles can dominate joint equilibrium: it is not absolute force that determines the result, but the relationship between intensity and angulation [5,7].
In cases where a diagonal force and a longitudinal force parallel to the segment act together, the latter cannot balance the transverse component of the oblique force [5,15]. The only possibility for longitudinal muscles to oppose is to express intensities sufficient to stiffen the structure itself in compression [3,15].
5.1 Clinical Example: Latissimus Dorsi and Paraspinal Muscles
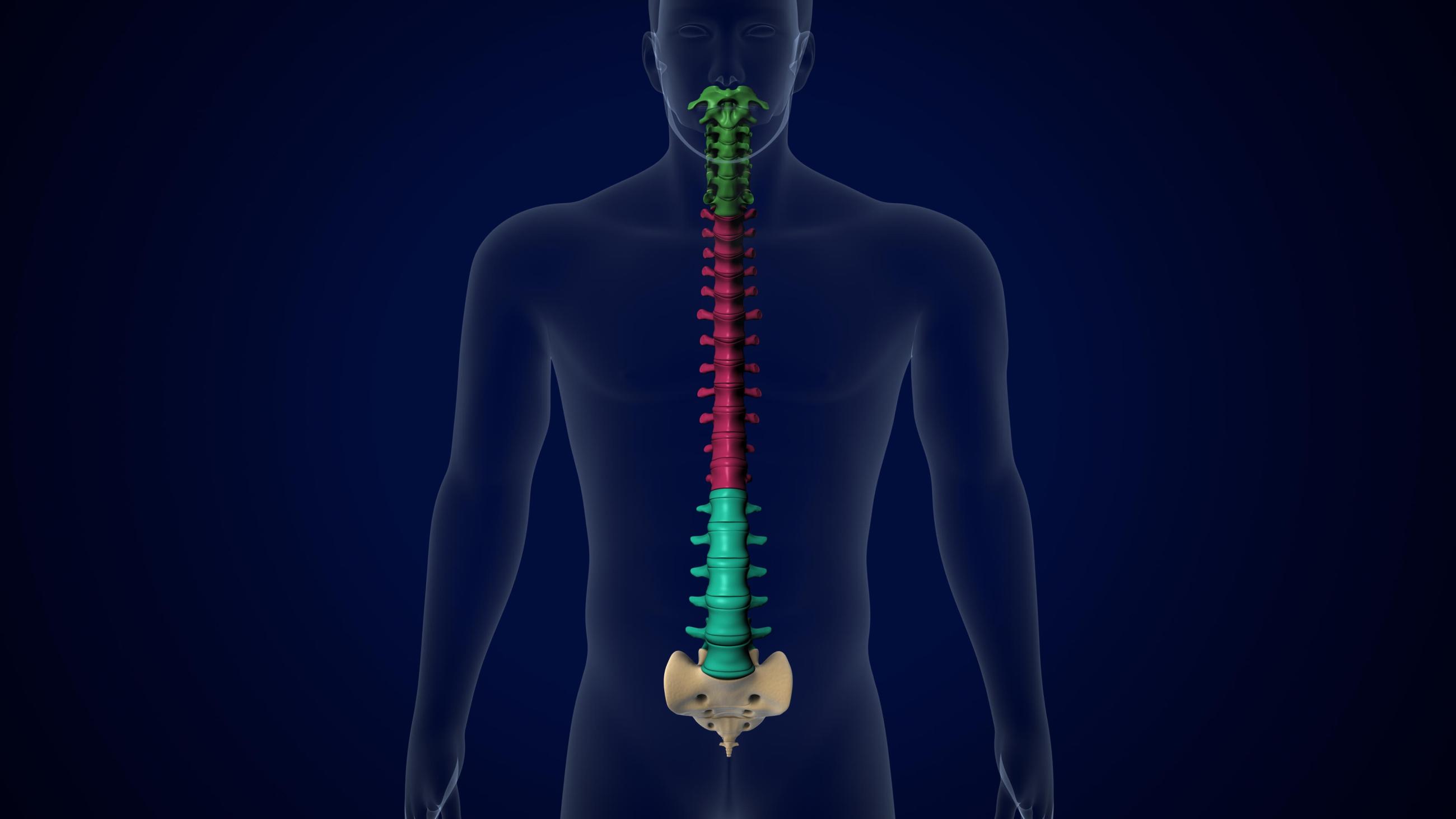
A clinical example concerns the relationship between the latissimus dorsi and paraspinal muscles in the thoracolumbar region [15,17].
The latissimus dorsi, with its insertions on the iliac crest, spinous processes from T7 to L5, and humerus, possesses fibres with oblique orientation relative to the vertebral column [12,17]. The horizontal component of its force vector tends to pull the vertebrae laterally.
The paraspinal muscles, conversely, have a predominantly longitudinal orientation, parallel to the spine [17,19]. For the geometric reasons explained above, the longitudinal vectors of the paraspinals cannot directly balance the horizontal component of the latissimus dorsi vector [15,17].
To prevent lateral deviation of the spine, the paraspinals have only one available strategy: to express very high-intensity vectors that stiffen the spine in axial compression, mechanically locking it [15,18]. This stiffening has a cost: it increases compression on the intervertebral discs and reduces segmental mobility [18,19].
This example illustrates an important clinical principle: electromyographic activity does not necessarily reflect the primary cause of the problem [17,19]. An EMG investigation would show low activity of the latissimus dorsi and intense activity of the paraspinals. The interpretation might suggest that the paraspinals are "hyperactive" and should be relaxed, or that the latissimus dorsi is "weak" and should be strengthened [17].
Vector analysis suggests the opposite interpretation: it is the shortening of the latissimus dorsi (with low EMG activity but high passive resistant force) that causes the problem, while paraspinal hyperactivity is a compensatory response necessary to maintain spinal verticality [1,17,19]. The correct intervention is not to relax the paraspinals nor to strengthen the latissimus dorsi, but to reduce the shortening of the connective components of the latissimus dorsi [1,4].
Spinal Verticality
6. Vectorial Dominances and Anatomical Asymmetries
In almost all joints, muscular forces are vectorially asymmetric [7,12]. This asymmetry is not pathological: it is an intrinsic anatomical characteristic of the human musculoskeletal system [12,20].
With respect to skeletal resultants, dominant and subdominant muscular actions are distinguished [4,13]. Dominance depends not only on the absolute force of the muscle, but on the combination of: number of muscles acting in the same direction; length of vectors (longer muscles generally have more powerful vectors); obliquity of lines of force relative to the skeletal segment [7,12,20].
6.1 Clinical Example: Shoulder Rotators
In the scapulohumeral relationship, the muscles that determine humeral internal rotation are anatomically dominant over those that determine external rotation [12,20].
The humeral internal rotators include: latissimus dorsi, pectoralis major, subscapularis, and teres major. The external rotators are: supraspinatus (with limited rotational component), infraspinatus, and teres minor [12,16]. The difference is evident: the internal rotators are greater in number, have larger muscle masses, and possess longer and more oblique vectors [12,20].
The vectorial resultant of the internal rotators, if these express high intensity (through active contraction or through connective shortening), cannot be balanced by the vectorial resultant of the external rotators [20,21]. This intrinsic asymmetry explains why humeral internal rotation with anteriorisation of the humeral head is one of the most frequent patterns in subacromial impingement syndromes [20,21].
Anatomical vectorial dominances become particularly evident in neurological conditions such as spastic hemiparesis [14,22]. In these conditions, the loss of supraspinal inhibitory control allows intrinsic dominances to manifest fully, without central nervous system modulation [22]. A hemiplegic patient is rarely observed with the humerus in spontaneous external rotation, precisely because the internal rotators are anatomically dominant [20,22].
Although the neurophysiological mechanisms of spasticity differ from physiological muscle shortenings [1,22], both conditions reveal the same anatomical reality: intrinsic vectorial asymmetries exist that, when not balanced by neural control or when altered by shortenings, determine predictable patterns of joint alteration [1,4,13].
We hope this article was helpful. For more information from AIFiMM Formazione, please visit their CPD Member Directory page. Alternatively, you can go to the CPD Industry Hubs for more articles, courses and events relevant to your Continuing Professional Development requirements.
References
1. Lastrico M. Clinical Assessment of Muscle Shortening. The CPD Certification Service; 2025.
2. Lastrico M. Body Equilibrium – A Physical-Clinical Interpretation of Human Upright Stability. The CPD Certification Service; 2025.
3. Winter DA. Biomechanics and Motor Control of Human Movement. 4th ed. Hoboken: Wiley; 2009.
4. Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndromes. St. Louis: Mosby; 2002.
5. Knudson D. Fundamentals of Biomechanics. 2nd ed. New York: Springer; 2007.
6. Zajac FE. Muscle and tendon: properties, models, scaling, and application to biomechanics and motor control. Crit Rev Biomed Eng. 1989;17(4):359-411.
7. Lieber RL, Ward SR. Skeletal muscle design to meet functional demands. Philos Trans R Soc Lond B Biol Sci. 2011;366(1570):1466-1476.
8. Fung YC. Biomechanics: Mechanical Properties of Living Tissues. 2nd ed. New York: Springer; 1993.
9. Herzog W. Skeletal muscle mechanics: questions, problems and possible solutions. J Neuroeng Rehabil. 2017;14(1):98.
10. Halliday D, Resnick R, Walker J. Fundamentals of Physics. 10th ed. Hoboken: Wiley; 2013.
11. Tipler PA, Mosca G. Physics for Scientists and Engineers. 6th ed. New York: W. H. Freeman; 2008.
12. Lieber RL, Fridén J. Functional and clinical significance of skeletal muscle architecture. Muscle Nerve. 2000;23(11):1647-1666.
13. Page P, Frank CC, Lardner R. Assessment and Treatment of Muscle Imbalance: The Janda Approach. Champaign: Human Kinetics; 2010.
14. Shumway-Cook A, Woollacott M. Motor Control: Translating Research into Clinical Practice. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2012.
15. Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383-389.
16. Cools AM, Declercq GA, Cambier DC, Mahieu NN, Witvrouw EE. Trapezius activity and intramuscular balance during isokinetic exercise in overhead athletes with impingement symptoms. Scand J Med Sci Sports. 2007;17(1):25-33.
17. McGill SM. Low Back Disorders: Evidence-Based Prevention and Rehabilitation. 3rd ed. Champaign: Human Kinetics; 2016.
18. Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31(18):2151-2161.
19. Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine: implications for injury and chronic low back pain. Clin Biomech. 1996;11(1):1-15.
20. Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech. 2003;18(5):369-379.
21. Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000;80(3):276-291.
22. Gracies JM. Pathophysiology of spastic paresis. I: Paresis and soft tissue changes. Muscle Nerve. 2005;31(5):535-551.
23. Janda V. Muscles and motor control in cervicogenic disorders: assessment and management. In: Grant R, editor. Physical Therapy of the Cervical and Thoracic Spine. New York: Churchill Livingstone; 1994. p. 195-216.
24. Gajdosik RL. Passive extensibility of skeletal muscle: review of the literature with clinical implications. Clin Biomech. 2001;16(2):87-101.
25. Trudel G, Uhthoff HK. Contractures secondary to immobility: is the restriction articular or muscular? An experimental longitudinal study in the rat knee. Arch Phys Med Rehabil. 2000;81(1):6-13.
26. Cuthbert SC, Goodheart GJ Jr. On the reliability and validity of manual muscle testing: a literature review. Chiropr Osteopat. 2007;15:4.
27. Kisner C, Colby LA, Borstad J. Therapeutic Exercise: Foundations and Techniques. 7th ed. Philadelphia: F.A. Davis; 2017.
28. Weppler CH, Magnusson SP. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther. 2010;90(3):438-449.